“Words are one of the most powerful devices we have to push ideas forward and have them adopted” –Nancy Duarte in her book DataStory.
If strategy is a car, content would be the tires.
High-quality tires are important because they bear the weight of the entire car. Since tires (just like shoes) touch the ground, they’re they only things that cushion us from the gravitational pull of our planet. So they better be good!
Using up 7.5 hours at the desk is very easy. But how much of that work actually benefited my team, my organization, customers, patients, or even myself?
What work am I hiding from when I’m doing aimless work?
If I don’t ask why I have this [[position, project, client, or relationship with a customer]], then I shouldn’t ask why I don’t have it anymore when it is taken away from me.
Most people who want to move up the food chain try to forge the actions of those who’ve made it: “if I do what they did, surely I will get to where they are.”
I question the validity of that because what worked THEN might be outdated NOW because situations have changed.
As Francis Bacon declared roughly five hundred years ago, “He that will not apply new remedies must expect new evils: for time is the greatest innovator.”
Instead of following WHAT they did, it might be more worthwhile to ask: “WHY did it work for them?”
It’s easy to hide behind proven ways, but it takes a brave soul to try new ways.
When soliciting input from team members, they generously dump information into a large heap. This information can come in many forms: verbal direction, emails, references, slides,….
Information doesn’t move people, but stories do.
This is why a writer takes on the assiduous work of going in to sort through the pile. Decluttering and then finding a place for the remaining information.
Samuel Langley, an intelligent and famous university professor, was working hard to invent a flying machine. Even the U.S. government betted on his success by awarding him a hefty grant.
Meanwhile, 2 uneducated men were working on the same problem. Neither had a college degree—not to mention internet access or university laboratory. These are the Wright brothers–and the rest is history.
So the next time I THINK I’m handed nothing more than a shoestring to fulfill the strategy/business goal/vision/…, I ALREADY possess the necessary assets.
Doing more with less works better than doing less with more. Relentless pursuit demands a strong sense of purpose.
Nailing a presentation to executives can open so many doors because these people have strong influence.
In the quick moment granted to me, how can I win their hearts and give them all the information that THEY need?
If only there was a template for presentations to executives! Something that someone actually took the time to think through and has proven time and time again that it works.
There is!
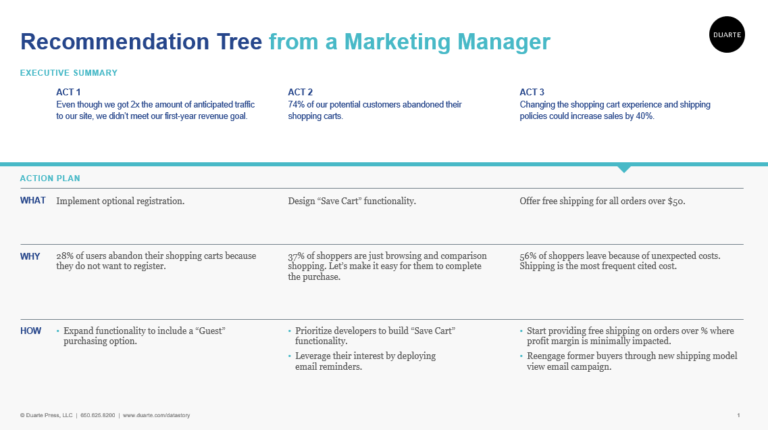
Check out Duarte Inc.’s template for an Executive Summary slide. They call this a “Recommendation Tree,” which, in Market Access language, is an Executive Summary slide for a presentation on RECOMMENDATIONS (it doesn’t work for value propositions, but it is godsend for recommendations).
What if there was no one else behind me to pick up the slack?
The possibilities magically line up when a gun is pointed at the head (figuratively, of course) because it’s now MY problem and ‘no’ is no longer an acceptable answer.
Everyone is granted 24 hours in a day. Yet why does it seem that some people are given extra time?
Mental intensity and time management hacks are both important.
Morning routine is like my oxygen mask. When I take care of myself, I can take care of others.
Once I reach my desk:
To-do list gives a framework for the day. When each item is given a time slot, it’s amazing how many things can be checked off in a single day!
Productive music (music without lyrics—just the beats) helps the mind from wandering off.
Short breaks at the end of the hour help to keep the creative juices flowing and also save the back.
3 words: I will die (one of the biggest lessons COVID-19 has taught me). When it’s my turn, I will only take 3 assets with me: mind, intellect, and soul. So if I’m spending 50% of my waking day at work, it better count!